Pharmacotherapeutic group: Drugs for acid-related disorders, proton pump inhibitor.
Pharmacology: Pharmacodynamics: Mechanism of Action: Esomeprazole is a weak base and is concentrated and converted to the active form in the highly acidic environment of the secretory canaliculi of the parietal cell, where it inhibits the enzyme H+K+-ATPase C the acid pump and inhibits both basal and stimulated acid secretion.
Pharmacodynamic effects: After 5 days of oral dosing with 20 mg and 40 mg of esomeprazole, intragastric pH above 4 was maintained for a mean time of 13 hours and 17 hours respectively, over 24 hours in symptomatic GERD patients. The effect is similar irrespective of whether esomeprazole is administered orally or intravenously.
Using AUC as a surrogate parameter for plasma concentration, a relationship between inhibition of acid secretion and exposure has been shown after oral administration of esomeprazole.
During intravenous administration of 80 mg esomeprazole as a bolus infusion over 30 minutes followed by a continuous intravenous infusion of 8 mg/h for 23.5 hours, intragastric pH above 4, and pH above 6 was maintained for a mean time of 21 hours and 11-13 hours, respectively, over 24 hours in healthy subjects.
Healing of reflux oesophagitis with esomeprazole 40 mg occurs in approximately 78% of patients after 4 weeks, and in 93% after 8 weeks of oral treatment.
During treatment with antisecretory medicinal products, serum gastrin increases in response to the decreased acid secretion. Also CgA increases due to decreased gastric acidity. The increased CgA level may interfere with investigations for neuroendocrine tumours.
Available published evidence suggests that proton pump inhibitors should be discontinued between 5 days and 2 weeks prior to CgA measurements. This is to allow CgA levels that might be spuriously elevated following PPI treatment to return to reference range.
An increased number of ECL cells possibly related to the increased serum gastrin levels, have been observed in both children and adults during long-term treatment with orally administered esomeprazole. The findings are considered to be of no clinical significance.
During long-term oral treatment with antisecretory drugs, gastric glandular cysts have been reported to occur at a somewhat increased frequency. These changes are a physiological consequence of pronounced inhibition of acid secretion, are benign and appear to be reversible.
Decreased gastric acidity due to any means including proton pump inhibitors, increases gastric counts of bacteria normally present in the gastrointestinal tract. Treatment with proton pump inhibitors may lead to slightly increased risk of gastrointestinal infections such as Salmonella and Campylobacter and, in hospitalised patients, possibly also
Clostridium difficile.
Paediatric population: Results from the paediatric studies further show that 0.5 mg/kg and 1.0 mg/kg esomeprazole in <1 month old and 1 to 11 month old infants, respectively, reduced the mean percentage of time with intra-oesophageal pH <4.
The safety profile appeared to be similar to that seen in adults.
In a study in paediatric GERD patients (<1 to 17 years of age) receiving long-term PPI treatment, 61% of the children developed minor degrees of ECL cell hyperplasia with no known clinical significance and with no development of atrophic gastritis or carcinoid tumours.
Pharmacokinetics: Distribution: The apparent volume of distribution as steady state in healthy subjects is approximately 0.22 l/kg body weight. Esomeprazole is 97% plasma protein bound.
Metabolism: Esomeprazole is completely metabolised by the cytochrome
P450 system (CYP). The major part of the metabolism of esomeprazole is dependent on the polymorphic CYP2C19, responsible for the formation of the hydroxy- and desmethyl metabolites of esomeprazole. The remaining part is dependent on another specific isoform, CYP3A4, responsible for the formation of esomepraole sulphone, the main metabolite in plasma.
Elimination: The parameters as follows reflect mainly the pharmacokinetics in
individuals with a functional CYP2C19 enzyme, extensive metabolisers.
Total plasma clearance is about 17 l/h after a single dose and about 9 l/h after repeated administration. The plasma elimination half-life is about 1.3 hours after repeated once daily dosing.
Esomeprazole is completely eliminated from plasma between doses with no tendency for accumulation during once daily administration.
The major metabolites of esomeprazole have no effect on gastric acid secretion. Almost 80% of an oral dose of esomeprazole is excreted as metabolites in the urine, the remainder in the faeces. Less than 1% of the parent drug is found in urine.
Linearity/non-linearity: Total exposure (AUC) increases with repeated administration of esomeprazole. This increase is dose-dependent and results in a non-linear dose-AUC relationship after repeated administration. This time- and dose-dependency is due to a decrease of first pass metabolism and systemic clearance probably caused by inhibition of the CYP2C19 enzyme by esomeprazole and/or its sulphone metabolite.
Following repeated doses of 40 mg administered as intravenous injections, the mean peak plasma concentration is approx. 13.6 micromol/l. The mean peak plasma concentration after corresponding oral doses is approx. 4.6 micromol/l. A smaller increase (of approx 30%) can be seen in total exposure after intravenous administration compared to oral administration. There is a dose linear increase in total exposure following intravenous administration of esomeprazole as a 30-minute infusion (40 mg or 80 mg) followed by a continuous infusion (4 mg/h or 8 mg/h) over 23.5 hours.
Special patient populations: Poor metabolisers: Approximately 2.9 ±1.5% of the population lacks a functional CYP2C19 enzyme and is called poor metabolisers. In these individuals, the metabolism of esomeprazole is probably mainly catalysed by CYP3A4. After repeated once daily administration of 40 mg oral esomeprazole, the mean total exposure was approximately 100% higher in poor metabolisers than in subjects with a functional CYP2C19 enzyme (extensive metabolisers). Mean peak plasma concentrations were increased
by about 60%. Similar differences have been seen for intravenous administration of esomeprazole. These findings have no implications for the posology of esomeprazole.
Hepatic impairment: The metabolism of esomeprazole in patients with mild to moderate liver dysfunction may be impaired. The metabolic rate is decreased in patients with severe liver dysfunction resulting in a doubling of the total exposure of esomeprazole. Therefore, a maximum dose of 20 mg should not be exceeded in GERD patients with severe dysfunction. For patients with bleeding ulcers and severe liver impairment, following an initial bolus dose of 80 mg, a maximum continuous intravenous infusion dose of 4 mg/h for 71.5 hours may be
sufficient. Esomeprazole or its major metabolites do not show any tendency to accumulate with once daily dosing.
Renal impairment: No studies have been performed in patients with decreased renal function. The metabolism of esomeprazole is not expected to be changed in patients with impaired renal function.
Elderly: The metabolism of esomeprazole is not significantly changed in elderly subjects (71-80 years of age).
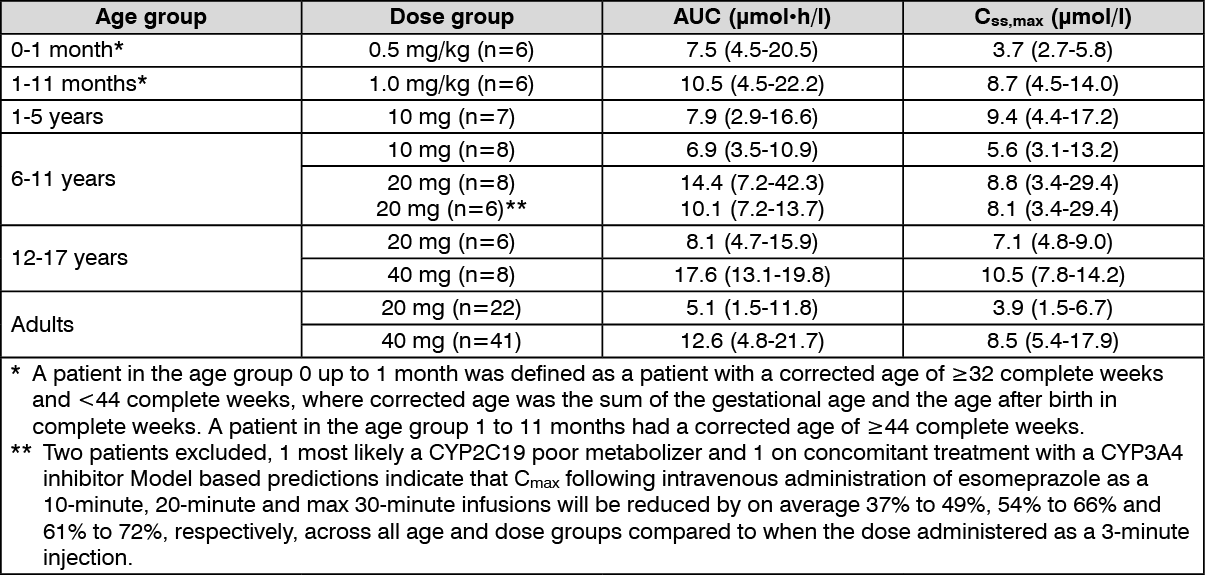
Paediatric population: In a randomized, open-label, multi-national, repeated dose study, esomeprazole was given as a once-daily 3-minute injection over four days. The study included a total of 59 paediatric patients 0 to 18 years old of which 50 patients (7 children in the age group 1 to 5 years) completed the study and were evaluated for the pharmacokinetics of esomeprazole.
The table as follows describes the systemic exposure to esomeprazole following the intravenous administration as a 3-minute injection in paediatric patients and adult healthy subjects. The values in the table are geometric means (range). The 20 mg dose for adults was given as a 30-minute infusion. The C
ss, max was measured 5 minutes post-dose in all paediatric groups and 7 minutes post-dose in adults on the 40 mg dose, and after stop of infusion in adults on the 20 mg dose.
(See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out